

When struggling with a mental health disorder, the path to improvement often begins with the lengthy process of trying various treatments and approaches to find the one that fits you best. So imagine the frustration if, after years of false starts and a frustrating lack of progress, you learn that you were misdiagnosed in the first place.
The rest of this article is behind a paywall. Please sign in or subscribe to access the full content.This is the unfortunate reality for many individuals with bipolar disorder (BP), as a wide overlap in symptoms often causes the condition to masquerade as depression – aka major depressive disorder (MDD). An estimated 60 percent of patients with BP are initially misdiagnosed with MDD and the time to a correct diagnosis is commonly several years to a decade.
Yet new work led by researchers from the University of Sydney suggests that a simple test using existing brain scanning technology could be used to distinguish the two disorders with a high degree of accuracy, and may even open the door for much-needed insights into their neurological origins.
"These two illnesses are virtually identical except that in bipolar individuals also experience mania,” lead investigator Dr Mayuresh Korgaonkar said in a statement, adding that BP frequently first onsets with a depressive phase.
"The wrong diagnosis can be dangerous, leading to poor social and economic outcomes for the patient as they undergo treatment for a completely different disorder. Identifying brain markers that could reliably tell them apart would have immense clinical benefit.”
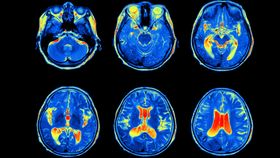
Hoping to do just that, Korgaonkar and his colleagues turned to functional magnetic resonance imaging (fMRI), a brain activity measurement that detects changes in blood flow. Past studies with fMRI have shown that the amygdala – the brain’s emotion processing center – activates differently in response to emotional stimuli (such as photos of human faces) in MDD and BP individuals compared with healthy individuals.
Furthermore, some earlier research has yielded patterns that could help mental health professionals differentiate between the two disorders. But, as the team notes in their paper, published in Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, all the previous investigations have used patients who were experiencing a depressive episode at the time – and the diagnostic power was inconsistent.

For their study, Korgaonkar’s group only enrolled people who were in remission at the time of the experiment, thus enabling them to look for differences in the underlying brain wiring of the two disorders rather than simply examining how a depressive episode affects the response to emotional stimuli. Twenty-three people with confirmed BP and 25 people with confirmed MDD who were matched for age, gender, and number and severity of depressive episodes were included, as well as 25 age and gender-matched healthy controls.
While inside an fMRI machine, all subjects were shown a series of images of faces with angry, disgusted, fearful, sad, happy, or neutral expressions. The photo series was presented at two speeds to account for both conscious and subliminal processing: 0.5 seconds per image with 0.75-second intervals between each for the former, and 0.01 seconds followed by 0.15 seconds of a neutral face with a 1.1-second interval for the latter.
An analysis of the scans revealed that the left side of the amygdala is less active and has reduced connectivity to other brain regions in people with BP compared with those with MDD. The presence of these markers predicted whether a brain scan belonged to a person with BP with 80 percent accuracy.
The team has already initiated a phase 2 trial to see if these promising findings can be replicated in a larger patient group.